Healthcare Financial Model Template
Model patient volume by payer, forecast provider revenue based on RVU production, and track accounts receivable — built for private practices, clinics, and medical groups.
What's Inside This Healthcare Financial Model Template
This template includes 8 worksheets, each designed for a specific part of your healthcare financial workflow:
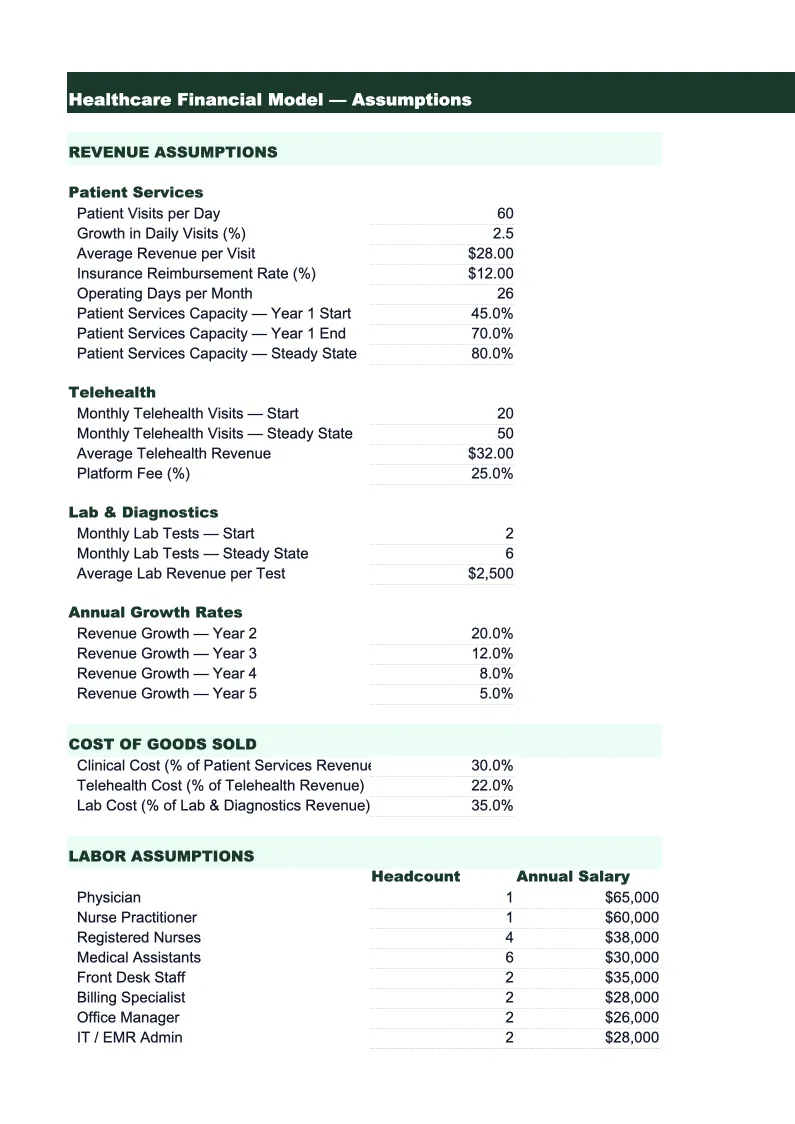
Assumptions
The central control sheet where you enter your practice's key operating parameters.
Patient Volume & Revenue
A 24-month patient volume and gross revenue schedule broken down by provider and payer type.
Payer Mix & Reimbursement
A detailed breakdown of revenue by payer and CPT code category.
Provider Staffing & RVU Model
A productivity and cost model for each clinical provider.
Expenses & Overhead
A monthly detail of all practice operating expenses not directly tied to individual providers.
Accounts Receivable
A monthly AR aging and cash collections model — one of the most important sheets for any healthcare practice.
P&L
A 24-month income statement built from the revenue, staffing, and overhead sheets.
KPI Dashboard
A one-page visual summary of the operational and financial metrics that practice managers, medical directors, and healthcare lenders review most closely.
Healthcare Financial Model Template Features
- Payer mix model separating Medicare, Medicaid, commercial insurance, and self-pay revenue with reimbursement rates by payer
- Provider productivity tracking using wRVU methodology with MGMA benchmark comparisons by specialty type
- Accounts receivable aging model with days-in-AR and net collection rate calculations by payer and aging bucket
- 24-month patient volume and revenue schedule with no-show rate, visit-type mix, and fee schedule inputs
- Provider-level contribution model showing net revenue per provider versus fully loaded provider cost including malpractice and benefits
- KPI dashboard with days in AR, net collection rate, overhead percentage, and wRVU productivity trends
How to Use This Healthcare Financial Model Spreadsheet
Start with the Assumptions sheet. Enter your provider roster, average visits per day per provider, and your payer mix percentages based on last year's actual claims data — your billing system or clearinghouse can pull this by payer in about 10 minutes. If you don't have exact figures, use your Medicare Explanation of Benefits and commercial remittances to estimate reimbursement per visit by payer type. Enter your net collection rate by payer — if you're unsure, 95–97% is a reasonable starting point for commercial payers, 90–93% for Medicare, and 70–80% for Medicaid depending on your state. Set your no-show and cancellation rate from your scheduling data. These inputs are the foundation that drives every revenue figure downstream.
With the assumptions in place, move to the Provider Staffing & RVU Model sheet and enter each provider's visit schedule and visit-type mix. Review the wRVU targets against the MGMA benchmarks shown — if a provider is projected to produce significantly fewer wRVUs than the median for their specialty, that's worth understanding before you finalize the model. Then work through the Expenses & Overhead sheet using last year's actual expenses as your baseline, adjusting for any planned changes: a new hire, a lease renewal, a transition to a new EMR. The AR sheet will model your collections timing automatically once revenue is set up. Your first complete model review should take 60–90 minutes total.
15 minutes from download to your first revenue projection
Download the template, enter your provider roster and payer mix, and see your practice's full financial picture — collections, AR aging, provider productivity, and overhead all in one place.
Why Every Medical Practice Needs a Financial Model
Medical practice finances are more complex than most small businesses because revenue is determined by three separate variables — visit volume, payer mix, and reimbursement rates — that all move independently of each other. A practice can increase visits by 10% and see revenue decline if the new patients skew toward Medicaid, which reimburses at 40–60% of commercial rates. It can hold volume steady and see revenue drop if a major commercial payer renegotiates rates at renewal. Without a model that separates these variables, a practice administrator can't tell whether a revenue shortfall came from fewer patients, a worse payer mix, declining collections performance, or a reimbursement rate change — and each of those causes requires a completely different response.
The financial metrics that define a healthy medical practice are distinct from other service businesses. Days in accounts receivable — how long it takes to collect a dollar of billed charges — should be under 35 days for a well-run practice; above 50 days typically signals billing workflow problems, excessive claim denials, or understaffed collections. Net collection rate, the percentage of net charges actually collected, should be 95–98% for commercial payers; below 92% means money is being written off that shouldn't be. Provider productivity measured in wRVUs per year provides a specialty-specific benchmark that eliminates the distortion of payer mix — a physician producing 5,200 wRVUs annually is performing similarly whether they're in a commercial-heavy suburban practice or a Medicaid-heavy safety-net clinic. These are the numbers that practice consultants, healthcare lenders, and DSO acquisition teams use to evaluate financial health.
Healthcare Industry at a Glance
Financial templates built for healthcare practices — from private clinics and therapy offices to specialty practices and medical groups. Pre-loaded with billing categories, insurance reimbursement tracking, and healthcare-specific KPIs.
Revenue Drivers
- Insurance reimbursements
- Patient copays and coinsurance
- Out-of-pocket self-pay
- Capitation payments
Key Cost Categories
- Clinical staff salaries
- Administrative and billing staff
- Medical supplies
- Malpractice insurance
- EMR/EHR software
- Facility rent and occupancy
Typical Margins
Gross: 45-65% · Net: 10-25%
Seasonality
Higher patient volume in fall/winter flu season; slower in summer. End-of-year spike as patients meet deductibles.
Key Performance Indicators
Healthcare Financial Model Template FAQ
More Healthcare Templates
Healthcare Balance Sheet Template for Excel
$29
Healthcare Budget Template for Excel
$29
Healthcare Business Plan Template for Excel
$39
Healthcare Cash Flow Template for Excel
$29
Healthcare Expense Tracker Template for Excel
$29
Healthcare Income Statement Template for Excel
$29
Healthcare Invoice Template for Excel
$29
Healthcare KPI Dashboard Template for Excel
$29
Healthcare P&L Template for Excel
$29
Healthcare Pro Forma Template for Excel
$29
Healthcare Project Budget Template for Excel
$29
Healthcare Sales Forecast Template for Excel
$29
Healthcare Practice Valuation Template for Excel
$29
More Financial Model Templates
Healthcare Financial Model Template
$29